
Services
Research Market Trends reports, in-depth papers, and more
Explore our archive of market research, ranging from broad Market Trends reports to deep-dive papers and more, covering all things healthcare IT.
Advisory Service Team up with us by utilizing our premier offering
The Chilmark Advisory Service provides access to our entire library of research, monthly access with our expert analyst team, discounts on custom research and consulting packages, and more.
Lighthouse Program Research access for healthcare providers.
For our provider partners, the Lighthouse Program is a way to access our research via short bi-annual interviews with our analyst team. In exchange for telling us your perspective on using healthcare IT in your practice, gain access to Chilmark’s library of research.
Custom Work Contract us for your bespoke research project
Engage our team for a deep dive on a topic that needs more industry attention. We want to help with your research project.

Recent Articles and Research
Chilmark Media

HIMSS24: Back to Form but Haunted by Change Healthcare
Good luck trying to get noticed for anything other than AI or cybersecurity HIMSS24 was the first HIMSS national conference that I will have missed since I first attended in 2012. It felt weird not to be there with all my friends and colleagues, and I certainly missed...

Providence’s Blueprint for Value Based, Data Driven Healthcare feat. Deepak Sadagopan
In this Chilcast episode, John Moore sits down with Deepak Sadagopan, COO of Population Health at Providence and CEO of the Providence Medicare ACO, Health Connect Partners, to discuss the strategic imperatives for healthcare executives navigating the transition to value-based care (VBC).

ViVE 2024: Bridging the Health 2.0 – HIMSS Gap
Workforce / capacity issues and AI – and where the two meet – are still the two biggest topics on clinical executives’ minds right now at both ViVE 2024 and HAS24. Probably the first time I’ve seen the same primary focus two years in a row – historically we’ve always seen a new buzzword / hype topic every year…

Regulation as a forcing function for innovation feat. Micky Tripathi, HHS’ National Coordinator for Health IT
Creating economic value to drive collective action in a severely fragmented industry Key Takeaways Appropriately tailored regulation helps coordinate healthcare progress and serves as a forcing function for innovation and progress when natural economic incentives fall...
Building Responsible AI in Healthcare: A Journey into Automation, Ethics, and Trust
As the pace of AI adoption grows and the variety (and quality) of solutions expands in kind, it's more important than ever to have a strategy regarding the use of these technologies. Chilmark Research is excited to share our first eBook, Building Responsible AI in...
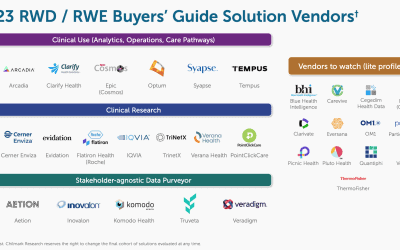
Real-World Data in Healthcare: 2023-2024 Buyers’ Guide
Coming 2024 Q1 Are you trying to navigate the dynamic landscape of healthcare technology? At Chilmark Research, we've developed our Buyers' Guide report format to empower decision-makers that are evaluating their options in the ever-evolving healthcare sector....
Chilmark Media

Providence’s Blueprint for Value Based, Data Driven Healthcare feat. Deepak Sadagopan

Regulation as a forcing function for innovation feat. Micky Tripathi, HHS’ National Coordinator for Health IT

Unlocking the Value of Data-Driven Healthcare with Keith Figlioli of LRVHealth

Empowering Patients with a Competitive Advantage feat. Grace Cordovano, PhD, BCPA
Our Clients
A sample of the organizations we’ve worked with over the years













Subscribe to the Chilmark Newsletter
Stay up to date with the latest healthcare IT news!